
Abstract
Psychiatric patients have become the focus of public attention, and current research suggests a possible link between Toxoplasma gondii (T. gondii) infection and mental illness. To understand the current situation of T. gondii infection in psychiatric patients in the study area, the relationship between T. gondii infection and mental diseases, and the influence of T. gondii infection on psychiatric patients, this study examined 3101 psychiatric inpatients from 2015 to 2020. All people included in the study were tested for anti-Toxoplasma IgM antibody and anti-Toxoplasma IgG antibody. Additionally, 4040 individuals from the general population were included as controls. The chi-square test and logistic regression analysis were carried out to determine the association between psychiatric disorders and T. gondii infection. The seroprevalence of anti-Toxoplasma IgM antibody was 0.23% (7/3101) in psychiatric inpatients and 0.11% (2/1846) in the general population, and there was no significant difference (p > 0.05). The seroprevalence rate of anti-Toxoplasma IgG antibodies was 3.03% (94/3101) in psychiatric inpatients and 1.05% (23/2194) in the general population, and there was a significant difference (p < 0.01). The seroprevalence of anti-Toxoplasma IgG antibody in psychiatric inpatients was significantly different between different age groups (p < 0.01). The positivity rate of anti-Toxoplasma IgG antibodies was 5.17% (3/58) in patients with mania, 3.24% (8/247) in patients with recurrent depressive disorder, 3.54% (13/367) in patients with depression, 3.22% (39/1213) in patients with schizophrenia, 2.41% (18/748) in patients with bipolar disorder and 2.25% (2/89) in patients with dissociative disorder. Compared to the general population, patients with mania (OR = 5.149 95% CI 1.501–17.659 p = 0.009), schizophrenia (OR = 3.136 95% CI 1.864–5.275 p = 0.000), depression (OR = 3.466 95% CI 1.740–6.906 p = 0.000), recurrent depressive disorder (OR = 3.160 95% CI 1.398–7.142 p = 0.006) and bipolar disorder (OR = 2.327 95% CI 1.249–4.337 p = 0.008) were found to be significantly associated with the seroprevalence of anti-Toxoplasma IgG antibody. This study suggests that the seroprevalence of T. gondii infection in psychiatric patients was higher and that age was an influencing factor of T. gondii infection in psychiatric patients. T. gondii infection was associated with mania, schizophrenia, depression, recurrent depressive disorder and bipolar disorder.
Similar content being viewed by others


Introduction
T. gondii is an obligate intracellular parasite with a worldwide distribution, and it is widely parasitic on the nucleated cells of humans and animals. T. gondii causes toxoplasmosis and infects about one third of the world's population1. This parasite is particularly common in developing countries, but it is also present in developed countries. Cats are the definitive hosts of T. gondii, while human, birds and reptiles are the intermediate hosts. T. gondii is mainly parasitic in the host's brain and muscle tissues, and T. gondii infection in humans is mainly caused by ingesting water and food contaminated by T. gondii or through vertical transmission from mother to child. When T. gondii infects people, it forms tissue cysts in some parts of the body, and these cysts can be reactivated when the immune function is weak2. Numerous studies suggest that T. gondii can alter human behaviour and increase its impact on public health3. Many studies have found a higher serological prevalence of T. gondii in psychiatric patients, which suggests that there may be a correlation between T. gondii infection and psychiatric disorders4. Current studies have focused on possible associations with T. gondii infection in schizophrenia, bipolar disorder and depression, but there are wide variations5. For example, studies have reported the seroprevalence of T. gondii among patients with schizophrenia (50.9%) and patients with bipolar disorders (52.6%)6. Other studies have reported that the anti-T. gondii IgG seropositivity rate was 18.8% among patients with bipolar disorders7.
The present study examined antibodies against T. gondii in psychiatric patients to determine the prevalence of T. gondii infection in psychiatric patients in the study area, identify the association between T. gondii infection and psychiatric disorders, and provide a theoretical basis and data-based support for the health administrative department in the region to formulate relevant prevention and control strategies for T. gondii infection among psychiatric patients.
Method
This was a cross-sectional study designed to assess the prevalence of T. gondii infection in psychiatric patients in the study area. Serum samples were collected from newly admitted psychiatric patients from 2015 to 2020 in Shandong Daizhuang Hospital, and the corresponding medical records were collected at the same time. This study obtained the informed consent of all participants and/or their legal guardians, as reflected in the medical records and medical orders. The inclusion criteria for psychiatric patients were as follows: (1) newly admitted inpatients, (2) diagnosed by a psychiatrist as mentally ill according to the International Classification of Diseases, 10th Revision, or The Diagnostic and Statistical Manual of Mental Disorders (DSM–5), and (3) available medical records. The exclusion criteria were as follows: patients with mental disorders due to alcohol/drug intoxication or abstinence, neurodevelopmental disorders, or traumatic and stress-related disorders. The doctor informed the patient according to the diagnosis and treatment process and issued a test application for anti-Toxoplasma antibodies. The patients were sent to the medical laboratory to provide blood samples. A total of 3101 psychiatric patients were included.
Additionally, a total of 4040 serum anti-Toxoplasma antibody test results were collected from individuals without psychiatric disorders at the Genetic Counselling Clinics and Physical Examination Center of the Affiliated Hospital of Jining Medical University or other companies. This included 1846 tests for anti-Toxoplasma IgM antibody and 2194 tests for anti-Toxoplasma IgG antibody. For privacy and other reasons in the general population, we only collected information about their age, except for Toxoplasma antibody test results. Participants in the study ranged in age from 9 to 77, the average age of psychiatric patients included in the study was 32.85 ± 10.76 years old, the average age of the general population tested for anti-Toxoplasma IgM antibodies was 32.33 ± 5.68 years old, and the average age of general people tested for anti-Toxoplasma IgG antibodies was 32.3 ± 5.77 years old.
This study collected medical records of inpatients with mental illness for further research. The positivity rate of anti-Toxoplasma IgM antibody was too low to perform an accurate statistical analysis; therefore, we analysed only the epidemiological characteristics of anti-Toxoplasma IgG antibody. Based on the collected medical records, the psychiatric inpatients were divided into a female group and a male group, with males accounting for the majority. The inpatients were divided into 3 groups based on age: 9–20 years old, 21–40 years old, and 41–77 years old. Han was the most common ethnicity, and individuals of other ethnicities accounted for approximately 1% of the sample. Marital status was categorized as single, married or divorced. According to their residence and surroundings, the inpatients were divided into rural and urban groups. Patients were also divided into six groups based on their occupation: jobless, farmer, worker, student, cadre and other groups. The population included in this study mainly came from Jining, Heze, Zaozhuang, Taian, Linyi and other regions, covering an area of approximately 53,000 square kilometres with a population of approximately 37.5 million. The terrain of the region includes plains, hills and mountains. According to the severity of mental illness, the inpatients were divided into a general group and a severe group. The severe group included patients with schizophrenia, schizoaffective disorder, bipolar disorder or other psychiatric disorders (excluding any substance-induced psychosis and unspecified psychosis) according to the International Classification of Diseases, 10th Revision or The Diagnostic and Statistical Manual of Mental Disorders (DSM–5). Based on existing research results classification and the type of mental illness diagnosed, people with mental illness are divided into seven groups: schizophrenia, bipolar disorder, depression, recurrent depressive disorder, dissociative disorder, mania and others (Table 1).
When patients arrived at the medical laboratory, they were informed of the purpose of drawing blood. Then, 5 ml of fasting blood was drawn from the subjects. The sample was centrifuged at 4000 r/min for 10 min, and then, the serum was separated for testing. Serological marker tests of T. gondii infection include anti-Toxoplasma IgM and IgG antibody measures using enzyme-linked immunosorbent assay (ELISA) (Auto Bio, China).
Statistical analysis was performed with SPSS v22 software (IBM Inc., Chicago, USA). Demographic characteristics were assessed with descriptive analysis. Pearson’s chi-square test, continuity correction, or Fisher's exact tests were performed for the analysis of categorical data. The putative risk factors were indicated by odds ratios (ORs) with 95% confidence intervals (95% CIs) using logistic regression, and a p value of < 0.05 was considered statistically significant.
Ethics approval and consent to participate
The research protocol was approved by the ethics committee of Shandong Daizhuang Hospital, and all experiments were performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations.
Results
As serological markers of T. gondii infection, anti-Toxoplasma IgG antibody presents latent exposure, and anti-Toxoplasma IgM antibody presents acute/recent exposure. The positivity rate of anti-Toxoplasma IgM antibody in psychiatric patients was 0.23% (7/3101), while in the general population, it was 0.11% (2/1846), with no statistically significant difference between the two groups (p = 0.359). The positivity rate of anti-Toxoplasma IgG antibody in psychiatric patients was 3.03% (94/3101), while in the general population, it was 1.05% (23/2194). There were statistically significant differences between the two groups, and psychiatric patients had a higher positivity rate than the general population (OR = 2.951, 95% CI 1.864–4.671, p = 0.000) (Table 2).
Through further analysis of anti-Toxoplasma IgG antibody in psychiatric patients, the results showed that there were significant differences in the positivity rates of anti-Toxoplasma IgG antibody among different age groups (χ2 = 12.234, p = 0.002). Compared with the 41–67 and 9–20 age groups, the 21–40 age group had the lowest positivity rate of anti-Toxoplasma IgG antibody, indicating that this age range was a potential protective factor (OR = 0.437, 95% CI 0.266–0.720, p = 0.001). There was no statistically significant difference in the positivity rates of anti-Toxoplasma IgG antibody in patients with various types of mental illness. There was no significant difference in the positivity rate of anti-Toxoplasma IgG antibody in the sex, ethnicity, marital status, residence, and severity groups (Table 3).
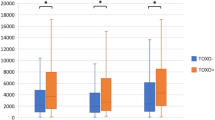
The positivity rate of anti-Toxoplasma IgG antibody in the general population was 0.00% (0/37) in the 9–20 years old age group, 1.08% (21/1946) in the 21–40 years old group and 0.95% (2/211) in the 41–77 years old group. The positivity rate of anti-Toxoplasma IgG antibody in the psychiatric patients was 3.04% (13/427) in the 9–20 years old age group, 2.32% (45/1942) in the 21–40 years old group and 4.90% (36/732) in the 41–77 years old group. By comparing the positivity rates of anti-Toxoplasma IgG antibody in the general population and psychiatric patients in different age groups, the results showed that the positivity rate of anti-Toxoplasma IgG antibody in the general population and psychiatric patients was significantly different between the 21–40 years old age group (p < 0.05) and 41–77 years old age group (p < 0.01) (Fig. 1).

Comparison of anti-Toxoplasma antibody-positivity rates between psychiatric patients and the general population in different age groups. Compared with the general population, psychiatric patients in the 21–40 years old age group (OR = 2.174 95% CI 1.290–3.664, p = 0.004) and 41–77 years old age group (OR = 5.405 95% CI 1.291–22.637 p = 0.021) had a higher positivity rate of anti-Toxoplasma IgG antibody.
A large number of studies have shown that patients with certain types of mental illness, such as schizophrenia, have a higher infection rate. This study compared various types of mental illness with the general population and found that compared to the general population, depression, recurrent depressive disorder, schizophrenia, and mania patients had a higher positivity rate of anti-Toxoplasma IgG antibody (Fig. 2). It is noteworthy that the positivity rate of anti-Toxoplasma IgG antibody was highest in patients with mania and recurrent depressive disorder.

Comparison of anti-Toxoplasma IgG antibody-positivity rates in different groups. Compared with general people, the values of different types of psychiatric disorders are dissociative disorder (OR = 2.170 95% CI 0.504–9.350 p = 0.299), bipolar disorder (OR = 2.327 95% CI 1.249–4.337 p = 0.008), schizophrenia (OR = 3.136 95% CI 1.864–5.275 p = 0.000), depression (OR = 3.466 95% CI 1.740–6.906 p = 0.000), recurrent depressive disorder (OR = 3.160 95% CI 1.398–7.142 p = 0.006), mania (OR = 5.149 95% CI 1.501–17.659 p = 0.009), and others (OR = 2.821 95% CI 1.364–5.837 p = 0.005).
Discussion
T. gondii infection is widespread around the world, recent studies have shown that the seroprevalence of anti-Toxoplasma antibody ranges from 10 to 80%. The seroprevalence of Toxoplasma infection in China is relatively low, ranging from 2.3% to 35.6% among different populations and geographic regions8. Numerous studies have found a higher serological prevalence of T. gondii infection in psychiatric patients9,10,11, and research on the relationship between T. gondii infection and psychiatric disorders has become a hot topic. China has a population of 1.4 billion, and the latest research12 shows that the weighted 12-month prevalence of mental disorders (excluding dementia) in China is 9.3% (95% CI 5.4–13.3), and the weighted lifetime prevalence is 16.6% (95% CI 13.0–20.2). Considering the large number of patients with mental illness in China, research on the epidemiological status of T. gondii infection and the association between mental illness and T. gondii infection is particularly important and necessary.
The results of the present study showed that the anti-Toxoplasma IgG and IgM antibodies in psychiatric patients and the general population were both at low levels in the study region8,13,14.
The positivity rate of anti-Toxoplasma IgG antibody in psychiatric patients was higher than that in the general population, which is similar to a previous study in Weihai, Shandong Province, between 2011 and 201313. The results indicate that psychiatric patients in the study area should pay attention to the detection of T. gondii infection. There was no significant difference in the positivity rates of anti-Toxoplasma IgM antibody between the general population and psychiatric patients, which indicates that there is no difference in acute/recent infection of T. gondii among the general population and psychiatric patients in this study area. The seroprevalence of anti-Toxoplasma antibody in psychiatric patients suggests that T. gondii infections in psychiatric patients in the study area are mostly recessive or long-term. However, the results are inconsistent with some research. Wang's research14 in Zhejiang, China, showed that seropositivity rates of anti-Toxoplasma IgG antibodies and anti-Toxoplasma IgM antibodies were both significantly higher in psychiatric patients than in the nonpsychiatric control group, which may indicate geographical differences in the epidemiological status of T. gondii infection in psychiatric patients.
In this study, the positivity rate of anti-Toxoplasma IgM antibodies in both the general population and patients with mental illness was lower than the results published in China (Chen et al., 2019; Pan, M., et al., 2017; Chen, X., et al., 2019.). This value is especially lower than the research results in the nearby area (Weihai) (Cong et al., 2015). A large number of investigations have focused on the association between T. gondii infection and psychiatric disorders, but the results of these studies are inconsistent. Numerous studies have reported that T. gondii seropositivity is related to mental illnesses such as schizophrenia, bipolar disorder, generalized anxiety disorder, obsessive–compulsive disorder, suicide, aggression, and impulsivity15,16,17,18. However, others have failed to demonstrate significant associations between psychiatric disorders and toxoplasmosis19,20. Anti-Toxoplasma IgM antibody is a marker of acute/recent exposure, persistent infection, or reinfection21, while previous studies have focused on anti-Toxoplasma IgG antibody, which is a marker of lifetime exposure or latent T. gondii infection and has a higher positivity rate than IgM antibody. The latest research found that chronic T. gondii infection leads to cortical neurodegeneration and results in the interaction of CX3CL1, complement and microglia, thereby dividing and clearing degenerate neurons22. Therefore, the analysis of anti-Toxoplasma IgG antibody in this study is more meaningful.
After further analysis and comparison of different types of mental illness, the present study found that Mania, schizophrenia, bipolar disorder, depression and recurrent depressive disorder were all associated with positivity rates of anti-Toxoplasma antibodies, except for dissociative depressive disorder. The seroprevalence of T. gondii infection in patients with bipolar disorder was significantly different from that in the general population, which is consistent with newly published meta-analysis results23,24. However, some articles7,19,25 suggest that bipolar disorder is not associated with T. gondii infection. Therefore, the relationship between bipolar disorder and T. gondii infection is still controversial, and more research is needed.
A large amount of research suggests a link between T. gondii infection and schizophrenia, T. gondii becoming a potentially relevant aetiological factor in some cases of schizophrenia26,27,28, and recent studies suggest that T. gondii infection may be an underlying component of the pathophysiology of schizophrenia29, which is consistent with our study, but there are also some studies that reach the opposite conclusion. More rigorous studies are needed from epidemiological studies to mechanistic studies to confirm the relationship between schizophrenia and T. gondii infection.
Most research showed an absence of an association between depression and T. gondii infection30,31,32. However, a potential association between depression/recurrent depressive disorder and T. gondii infection was found in this study, and the same result was also found in Alvarado-Esquivel's study 33,34. More research on the relationship between T. gondii infection and depression is needed to explain the different conclusions. Furthermore, T. gondii infection affects the susceptibility and severity of depression in children, adolescents and pregnant women35,36, and patients with depression should pay attention to T. gondii infection. This study found a potential association between mania and T. gondii infection, but the current research on the relationship between mania and T. gondii infection is still insufficient to draw definitive conclusions, and more attention should be given to mania patients.
Existing research has shown that people who live in rural areas are at increased risk for toxoplasmosis37, but no consistent results were found in our study. Studies have found differences in the seroprevalence of anti-Toxoplasma antibody between males and females with psychosis38, which is inconsistent with our study. More research is needed to explain these phenomena. In the present study, psychiatric patients had the lowest positivity rate of anti-Toxoplasma IgG antibody in the 21–40 age group, indicating that this age group had the lowest risk of T. gondii infection, which may be because of the strong body and immunity in this age group.
The subjects included in this study are mainly from the southwestern regions of Shandong Province and parts of Henan and Jiangsu Province, with a population of approximately 40 million in the study area. Shandong Daizhuang Hospital is the largest psychiatric specialized hospital in Shandong Province; therefore, this study can accurately reflect the status of T. gondii infection in psychiatric patients in the study area and, to a certain degree, even east of China. The present study is a cross-sectional study, and cohort studies should be conducted in the future to better explain the internal connection of psychiatric disorders and T. gondii infection.
The present study mainly analysed T. gondii infection in psychiatric inpatients due to the difficulty in collecting basic data from the general population and outpatient mental patients. The population density in this study area is high, and the sample size included is relatively small. Because only the age information of the general population is available, more detailed personal information of the general population cannot be obtained for further analysis, and investigations with a larger sample size and different population groups should be performed to evaluate multiple influencing factors. It is widely believed that pregnant women should not have cats39, but research indicates that cat ownership in pregnancy or early childhood does not confer an increased risk of later adolescent psychotic experiences40. The extent to which cats are associated with T. gondii infection in patients with mental illness should be confirmed in future studies. Previous studies have suggested that anti-Toxoplasma antibody seropositivity persists throughout life41, but as research on anti-Toxoplasma antibodies increases and population-based analyses, some studies have suggested that persistent exposure to T. gondii is required for the maintenance of antibody levels42; therefore, anti-Toxoplasma antibody testing should be used as a routine test for assessing infection status and treatment monitoring in patients with mental illness.
At present, there have been many studies on the relationship between T. gondii infection and psychiatric disorders, and there are still many controversies and uncertainties. First, the results are very different. This may be because different people in different regions will have different results. Second, it is difficult to determine and explain the causal relationship between T. gondii infection and psychiatric disorders. From the perspective of aetiology and pathogenic mechanism, it is assumed that T. gondii infection will cause mental illness. It is assumed from an epidemiological perspective that patients with mental illness are susceptible to T. gondii infection due to poor health awareness or lower immunity. Therefore, research on the relationship between psychiatric disorders and T. gondii infection should be analysed in detail.
In summary, the seropositivity rate of T. gondii or the infection rate of T. gondii in the population in this region is maintained at a low level, but the seropositivity rate of T. gondii or the infection rate of T. gondii in patients with mental illness is maintained at a higher level than that in the general population. Age and different types of mental illness may be associated with T. gondii infection. More scientific and rigorous research from populations and laboratories is needed in our study region to determine the relationship between T. gondii infection and psychiatric disorders, especially mania, schizophrenia, depression, and recurrent depressive disorder.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Ansari-Lari, M., Farashbandi, H. & Mohammadi, F. Association of Toxoplasma gondii infection with schizophrenia and its relationship with suicide attempts in these patients. Trop. Med. Int. Health TM & IH 22(10), 1322–1327 (2017).
Carruthers, V. B. & Suzuki, Y. Effects of Toxoplasma gondii infection on the brain. Schizophr. Bull. 33(3), 745–751 (2007).
Martinez, V. O., de Mendonca Lima, F. W., de Carvalho, C. F. & Menezes-Filho, J. A. Toxoplasma gondii infection and behavioral outcomes in humans: A systematic review. Parasitol. Res. 117(10), 3059–3065 (2018).
Morais, F. B., Arantes, T. & Muccioli, C. Seroprevalence and manifestations of ocular toxoplasmosis in patients with Schizophrenia. Ocul. Immunol. Inflamm. 27(1), 134–137 (2019).
Yalın Sapmaz, Ş, Şen, S., Özkan, Y. & Kandemir, H. Relationship between Toxoplasma gondii seropositivity and depression in children and adolescents. Psychiatry Res. 278, 263–267 (2019).
Hussein, E. A. M. et al. Seroprevalence of Toxoplasma gondii among patients with schizophrenia and bipolar disorder in Upper Egypt: A comparative study with a control group. Ann Parasitol. 66(2), 183–192 (2020).
Şirin, M. C., Kılıç, F., Demirdaş, A., Arıdoğan, B. & Sesli, Çetin. E. An investigation into the association between toxoplasma gondii infection and bipolar disorder. Turkiye parazitolojii dergisi 45(4), 241–246 (2021).
Pan, M., Lyu, C., Zhao, J. & Shen, B. Sixty years (1957–2017) of research on toxoplasmosis in China-An overview. Front. Microbiol. 8, 1825 (2017).
Fekadu, A., Shibre, T. & Cleare, A. J. Toxoplasmosis as a cause for behaviour disorders–overview of evidence and mechanisms. Folia parasitologica 57(2), 105–113 (2010).
Stepanova, E. V. et al. Toxoplasmosis and mental disorders in the Russian Federation (with special reference to schizophrenia). PloS one 14(7), e0219454 (2019).
Hamdani, N. et al. Immunoglobulin sub-class distribution in bipolar disorder and schizophrenia: Potential relationship with latent Toxoplasma Gondii infection. BMC Psychiatry 18(1), 239 (2018).
Huang, Y. et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 6(3), 211–224 (2019).
Cong, W. et al. Seroprevalence and associated risk factors of Toxoplasma gondii infection in psychiatric patients: A case-control study in eastern China. Epidemiol. Infect. 143(14), 3103–3109 (2015).
Chen, X. et al. Association between Toxoplasma gondii infection and psychiatric disorders in Zhejiang, Southeastern China. Acta Trop. 192, 82–86 (2019).
Akaltun, I., Kara, S. S. & Kara, T. The relationship between Toxoplasma gondii IgG antibodies and generalized anxiety disorder and obsessive-compulsive disorder in children and adolescents: A new approach. Nordic J. Psychiatry 72(1), 57–62 (2018).
Markovitz, A. A. et al. Toxoplasma gondii and anxiety disorders in a community-based sample. Brain Behav. Immun. 43, 192–197 (2015).
Mortensen, P. B. et al. Early infections of Toxoplasma gondii and the later development of schizophrenia. Schizophr. Bull. 33(3), 741–744 (2007).
Zhang, Y. et al. Toxoplasma gondii immunoglobulin G antibodies and nonfatal suicidal self-directed violence. J. Clin. Psychiatry 73(8), 1069–1076 (2012).
Avramopoulos, D. et al. Infection and inflammation in schizophrenia and bipolar disorder: A genome wide study for interactions with genetic variation. PloS one 10(3), e0116696 (2015).
De Witte, L. D. et al. The association between antibodies to neurotropic pathogens and schizophrenia: A case-control study. NPJ schizophrenia 1, 15041 (2015).
Monroe, J. M., Buckley, P. F. & Miller, B. J. Meta-analysis of anti-toxoplasma gondii IgM antibodies in acute psychosis. Schizophrenia Bull. 41(4), 989–998 (2015).
Li, Y., Severance, E. G., Viscidi, R. P., Yolken, R. H. & Xiao, J. Persistent toxoplasma infection of the brain induced neurodegeneration associated with activation of complement and microglia. Infect. Immun. https://doi.org/10.1128/IAI.00139-19 (2019).
de Barros, J. et al. Is there any association between Toxoplasma gondii infection and bipolar disorder? A systematic review and meta-analysis. J. Affective Disord. 209, 59–65 (2017).
Chaudhury, A. & Ramana, B. V. Schizophrenia and bipolar disorders: The Toxoplasma connection. Trop. Parasitol. 9(2), 71–76 (2019).
Alvarado-Esquivel, C., Estrada-Martinez, S. & Perez-Alamos, A. R. A case-control seroprevalence study on the association between toxoplasma gondii infection and bipolar disorder. Front. Psychiatry 10, 766 (2019).
Torrey, E. F., Bartko, J. J., Lun, Z. R. & Yolken, R. H. Antibodies to Toxoplasma gondii in patients with schizophrenia: A meta-analysis. Schizophrenia Bull. 33(3), 729–736 (2007).
Torrey, E. F., Bartko, J. J. & Yolken, R. H. Toxoplasma gondii and other risk factors for schizophrenia: An update. Schizophrenia Bull. 38(3), 642–647 (2012).
Wang, H. L. et al. Prevalence of Toxoplasma infection in first-episode schizophrenia and comparison between Toxoplasma-seropositive and Toxoplasma-seronegative schizophrenia. Acta Psychiatr. Scand. 114(1), 40–48 (2006).
Akgül, Ö. et al. Toxoplasma gondii infection by serological and molecular methods in schizophrenia patients with and without suicide attempts: An age-sex-matched case-control study. Int. J. Clin. Pract. 75(8), e14449 (2021).
Alvarado-Esquivel, C. et al. Lack of association between Toxoplasma gondii exposure and depression in pregnant women: A case-control study. BMC Infect. Diseases 17(1), 190 (2017).
Nayeri Chegeni, T. et al. Is there any association between Toxoplasma gondii infection and depression? A systematic review and meta-analysis. PloS one 14(6), e0218524 (2019).
de Bles, N. J. et al. Toxoplasma gondii seropositivity in patients with depressive and anxiety disorders. Brain Behav. Immunity Health 11, 100197 (2021).
Alvarado-Esquivel, C. et al. Toxoplasma gondii infection and depression: A case-control seroprevalence study. Eur. J. Microbiol. Immunol. 6(2), 85–89 (2016).
Alvarado-Esquivel, C. et al. Toxoplasma gondii infection and mixed anxiety and depressive disorder: A case-control Seroprevalence study in durango, Mexico. J. Clin. Med. Res. 8(7), 519–523 (2016).
Yalin Sapmaz, S., Sen, S., Ozkan, Y. & Kandemir, H. Relationship between Toxoplasma gondii seropositivity and depression in children and adolescents. Psychiatry Res. 278, 263–267 (2019).
Nourollahpour Shiadeh, M. et al. The correlation between Toxoplasma gondii infection and prenatal depression in pregnant women. Eur. J. Clin. Microbiol. Infect. Diseases 35(11), 1829–1835 (2016).
Gawor, J., Borecka, A., Zarnowska, H., Marczynska, M. & Dobosz, S. Environmental and personal risk factors for toxocariasis in children with diagnosed disease in urban and rural areas of central Poland. Vet. Parasitol. 155(3–4), 217–222 (2008).
Khademvatan, S., Khajeddin, N., Izadi, S. & Yousefi, E. Investigation of anti-Toxocara and anti-toxoplasma antibodies in patients with schizophrenia disorder. Schizophrenia Res. Treat. 2014, 230349 (2014).
Achaw, B. et al. Sero-prevalence of Toxoplasma gondii and associated risk factors among psychiatric outpatients attending University of Gondar Hospital, Northwest Ethiopia. BMC Infect. Diseases 19(1), 581 (2019).
Solmi, F., Hayes, J. F., Lewis, G. & Kirkbride, J. B. Curiosity killed the cat: No evidence of an association between cat ownership and psychotic symptoms at ages 13 and 18 years in a UK general population cohort. Psychological medicine 47(9), 1659–1667 (2017).
Rougier, S., Montoya, J. G. & Peyron, F. Lifelong persistence of toxoplasma cysts: A questionable dogma?. Trends Parasitol. 33(2), 93–101 (2017).
Yolken, R., Torrey, E. F. & Dickerson, F. Evidence of increased exposure to Toxoplasma gondii in individuals with recent onset psychosis but not with established schizophrenia. PLoS Negl. Trop. Diseases 11(11), e0006040. https://doi.org/10.4088/JCP.11m07532 (2017).
Acknowledgements
This work was supported by the Teachers' Scientific Research Support Fund of Jining Medical University [Number: JYFC2019FKJ028].
Author information
Authors and Affiliations
Contributions
T.L. carried out data collection and article writing, D.L. and D.B. carried out article design, and P.G. carried out data collection.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests. All authors agree to publish this work.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, T., Gao, P., Bu, D. et al. Association between Toxoplasma gondii infection and psychiatric disorders: a cross-sectional study in China. Sci Rep 12, 15092 (2022). https://doi.org/10.1038/s41598-022-16420-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16420-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
